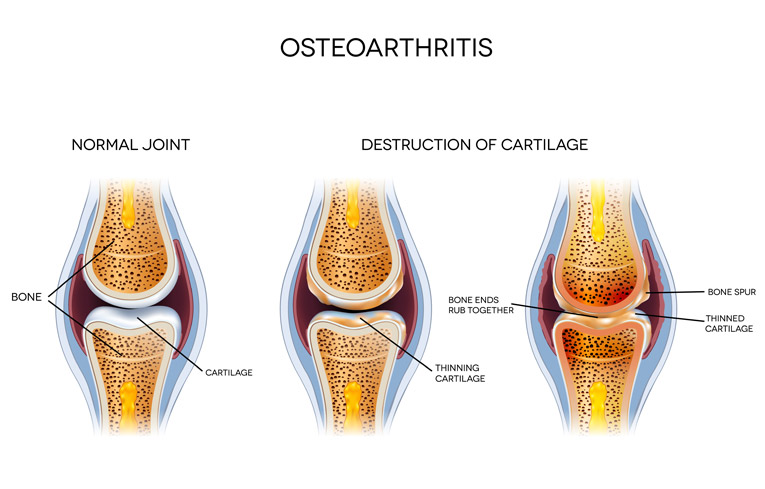
Arthritis refers to inflammation of a joint which can affect any of the important structures inside a joint, including the joint lining (synovium), bones, cartilage, or supporting tissues. Common symptoms include chronic arthritis pain, stiffness, and swelling of the joint. The condition may affect one or several joints throughout the body with knee joint pain being a common symptom. Degeneration of the cartilage can lead to destruction of the joint and the need for total joint replacement.
Etiologies of the Various Forms of Arthritis
Degenerative Arthritis (Osteoarthritis)
Degenerative arthritis, also known as ‘Osteoarthritis’ (OA), results from a complex interplay of multiple factors, including loss of joint cartilage integrity, genetics, local inflammation, abnormal alignment, excessive mechanical forces, and impaired cellular and biochemical processes. Loss of articular cartilage tissue results in an irregular joint bearing surface, which can impair joint function and the homeostasis of joint tissues.1 In patients with OA, there is an imbalance of breakdown and repair of tissues within a synovial joint. Thinning of cartilage is a normal consequence of aging, and it is important to remember that thinning of the cartilage layer is not pain-causing in and of itself and many patients can be pain-free despite having thin cartilage. In fact, painful OA can occur in younger patients where it is often a consequence of injury or overuse.
Hips, knees, hands and spines are the most commonly affected joints. Osteoarthritis is subdivided by etiology. In primary idiopathic OA, the origin of the disease is unknown and it progresses slowly over a period of years. In secondary OA, the disease is believed to be related to a specific inciting event such as trauma, other joint related disease, or congenital, developmental or endocrine disorders.2
Brandt K. Osteoarthritis: Clinical patterns and pathology. In: Textbook of Rheumatology, Fifth Edition, Kelley WN, Harris ED Jr, Ruddy S, Sledge CE (Eds), W.B. Saunders, Philadelphia 1997. p.1383
Altman R, Asch E, Bloch D, et al. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association. Arthritis Rheum 1986; 29:1039.
Post-Traumatic Arthritis
Post-traumatic arthritis occurs when an inciting trauma impacts the joint causing cartilage damage to the cartilage, ligaments or menisci. Examples could be a car crash, a sporting injury, or simply a fall. At times, a patient may experience swelling of the joint, pain, or even an inability to move that joint after the incident.1 Ligamentous instability (such as an anterior cruciate ligament tear) following traumatic injury can accelerate the arthritic process
U.S. National Library of Medicine. Posttraumatic Arthritis Accessed 12/1/2015
Inflammatory Arthritis
Rheumatoid Arthritis (RA) is an auto-immune disease, meaning that the patient’s own immune defenses attack the body. In this disease, immune cells called leukocytes (white blood cells) travel into the joint space and trigger an immunologic reaction, releasing inflammatory mediators leading to inflammation and tissue destruction. Warm, tender joints and morning stiffness lasting greater than 1 hour are very common symptoms for patients with rheumatoid arthritis. Patients can experience loss of energy and fevers due to inflammation occurring in the body.1
Psoriatic Arthritis: This type of inflammatory arthritis affects 0.3% to 1% of the population. Symptoms are present on not only joints, but also on the skin. Very similar to RA, this inflammatory arthritis has a genetic, immunologic, and environmental component. Patients develop joint pain, stiffness, and swelling along with silvery skin plaques and irritation. Often times, bones can weaken, causing joint destruction or even fusion, which can be identified on x-rays.2
"Rheumatoid Arthritis." National Institute of Arthritis and Musculoskeletal and Skin Diseases. National Institutes of Health, Aug. 2014. Web. 09 Dec. 2015.
Gladman, D. D., et al. "Psoriatic arthritis: epidemiology, clinical features, course, and outcome." Annals of the Rheumatic Diseases 64.suppl 2 (2005): ii14-ii17.
Gouty Arthritis
Gouty Arthritis is a condition that occurs after multiple episodes of gout. After several instances of gout, the joint can become damaged. Gout of the joints is due to the buildup of a molecule called uric acid, which the body naturally produces. It is characterized by sudden and extremely painful episodes in joints. Gout commonly occurs in the toe area, which is referred to as a podagra during episodes of severe inflammation. Consumption of high levels of protein and alcoholic beverages, or kidney failure leads to higher levels of uric acid in the blood which eventually deposit into joints. Over time this can lead to gouty arthritis. Another condition is calcium pyrophosphate deposition disease which is also called pseudo-gout and can cause similar findings to uric acid gout.
"1. Wallace SL, Robinson H, Masi AT, Decker JL, Mccarty DJ, Yü TF. Preliminary criteria for the classification of the acute arthritis of primary gout. Arthritis Rheum. 1977;20(3):895-900.
Reactive Arthritis
Reactive Arthritis is a type of arthritis that develops during or shortly after an infection elsewhere in the body. The most commonly identified pathogens are Chlamydia trachomatis, Yersinia, Salmonella, Shigella, and Campylobacter. It is also less commonly seen with E. Coli, Clostridium difficile, and Chlamydia pneumonia.1-5 Reactive arthritis often involves one or more joints, particularly in the lower extremities such as the knee, and it has an interval ranging from days to weeks between the arthritis and infection.6 Reactive arthritis often has a genetic predisposition and will not occur in all patients after these infections
Townes JM. Reactive arthritis after enteric infections in the United States: the problem of definition. Clin Infect Dis 2010; 50:247.
Rohekar S, Pope J. Epidemiologic approaches to infection and immunity: the case of reactive arthritis. Curr Opin Rheumatol 2009; 21:386.
Pope JE, Krizova A, Garg AX, et al. Campylobacter reactive arthritis: a systematic review. Semin Arthritis Rheum 2007; 37:48.
Hannu T. Reactive arthritis. Best Pract Res Clin Rheumatol 2011; 25:347.
Morris D, Inman RD. Reactive arthritis: developments and challenges in diagnosis and treatment. Curr Rheumatol Rep 2012; 14:390.
Braun J, Kingsley G, van der Heijde D, Sieper J. On the difficulties of establishing a consensus on the definition of and diagnostic investigations for reactive arthritis. Results and discussion of a questionnaire prepared for the 4th International Workshop on Reactive Arthritis, Berlin, Germany, July 3-6, 1999. J Rheumatol 2000; 27:2185.
Basic Anatomy
Cartilage
Cartilage is a shock-absorbing connective tissue that is found on the ends of bones. Lining in this area provides a near frictionless gliding surface and as a barrier to prevent bone on bone contact. Cartilage is primarily composed of collagen, which provides cartilage with its unique physical properties.1 In load-bearing areas such as the hips or knees, the erosion of cartilage and the lack of regeneration cause severe pain and decreased mobility that is associated with osteoarthritis.2 The hallmark of osteoarthritis is the loss of cartilage over time, leading to bone-on-bone contact associated with chronic pain and disability.3
Pratt, Rebecca. "Supporting Tissue: Cartilage".AnatomyOne. Amirsys, Inc. Retrieved 26 October 2012.
Hayes WC, Mockros LF. Viscoelastic properties of human articular cartilage. J Appl Physiol. 1971;31(4):562-8.
Arden N, Blanco F, Cooper C et al. Atlas of Osteoarthritis. Springer; 2015.
Synovial Fluid
Synovial fluid is the viscoelastic fluid that surrounds joint tissues. It provides lubrication and shock absorption, and allows movement to occur smoothly and painlessly.1 Hyaluronic acid, also known as hyaluronan or sodium hyaluronate, is the biopolymer responsible for the viscoelastic properties of synovial fluid. The concentration and quality of hyaluronic acid is diminished in joints afflicted by aging and inflammation, especially in patients with progressive osteoarthritis.2-4 Synovial fluid from osteoarthritic joints has a lower elasticity and viscosity when compared to normal joints.5-7 Intra-articular injections of hyaluronic acid is an FDA-approved treatment based on replacing the damaged synovial fluid with a more protective temporary substitute.
Hui AY, Mccarty WJ, Masuda K, Firestein GS, Sah RL. A systems biology approach to synovial joint lubrication in health, injury, and disease. Wiley Interdiscip Rev Syst Biol Med. 2012;4(1):15-37.
Band PA, Heeter J, Wisniewski HG, et al. Hyaluronan molecular weight distribution is associated with the risk of knee osteoarthritis progression. Osteoarthr Cartil. 2015;23(1):70-6.
Balazs EA, Watson D, Duff IF, Roseman S. Hyaluronic acid in synovial fluid: 1: molecular parameters of hyaluronic acid in normal and arthritic human fields. Arthritis Rheum 1967;10:357-76.
Larsen NE, Lombard KM, Parent EG, Balazs EA. Effect of hylan on cartilage and chondrocyte cultures. J Orthop Res. 1992;10(1):23-32.
Dahl LB, Dahl IMS, Engstrom-Laurent A, Granath K. Concentration and molecular weight of sodium hyaluronate in synovial fluid from patients with rheumatoid arthritis and other arthropathies. Ann Rheum Dis 1985;44:817-22. 5.
Hilbert BJ, Rowley G, Antonas KN. Hyaluronic acid concentration in synovial fluid from normal and arthritic joints of horses. Aust Vet J 1984;61:22-4. 6.
Sunblad L. Glycosaminoglycans and proteoglycans in synovial fluid. In: Balazs EA, Jeanloz RW, eds. The amino sugars: the chemistry and biology of compounds containing amino sugars. New York: Academic Press, 1965:229-50.
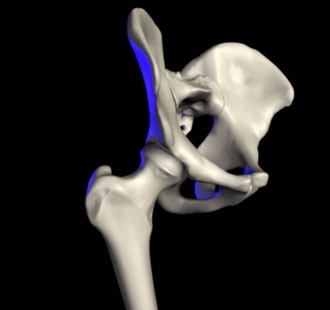
The Hip
The hip is one of the most flexible joints of the body. It is a ball and socket joint formed between the proximal end of the femur bone and the acetabulum (or the socket) of the pelvic bone. This allows us to move our legs in a wide range of motion for a number of activities.
The Knee
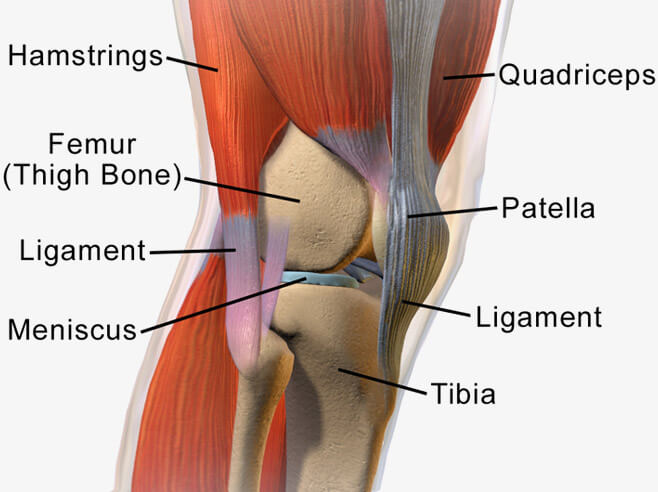
The knee is one of the strongest joints in the human body. The knee joint is also known as the tibiofemoral joint and is composed of three bones: the femur (thigh bone), the patella (knee cap), and the tibia (shin bone). Together, these bones come together to form a synovial hinge joint that allows flexion and extension of the leg.
What Are the Signs and Symptoms of degenerative arthritis?
Stages of Knee Osteoarthritis
The symptoms of Arthritis can vary greatly from person to person, but may include:
Pain, especially chronic arthritis pain, can be exacerbated by activity and relieved by rest.
Referred pain (also known as reflective pain) is when soreness occurs in a place that is not the source of the pain. For example, osteoarthritis in the hip can cause pain in the anterior thigh as well as leading to knee joint pain.
Stiffness after periods of inactivity. Morning stiffness is also very common but usually goes away within an hour of rising in individuals with osteoarthritis.
Joint swelling can occur when there is excess fluid accumulation in areas such as the knee further increasing any chronic arthritis pain.
Bone popping/cracking (or crepitus) can result from the development of bone spurs that are expressed as bony protuberances under the skin and around the joint.
The severity of degenerative arthritis is divided into 4 stages
Stage 1
Stage 2
Stage 3
Stage 4
Stage 1
A person with stage 1 degenerative arthritis exhibits very minor bone spur growth. (Bone spurs are boney growths that often develop where arthritic bones meet each other in the joint.) Likely, a person with stage 1 degenerative arthritis is not experiencing any pain or discomfort as a result of the very minor wear on the components of the joint.2
Stage 2
Considered a “mild” stage of the condition. X-rays of knee joints in this stage will reveal greater bone spur growth, but the cartilage likely remains at a healthy size — the space between the bones is normal, and the bones are not rubbing or scraping on one another. Synovial fluid is also typically still present at sufficient levels for normal joint motion. However, this is the stage where people may first begin experiencing symptoms — pain after a long day of walking or running, greater stiffness in the joint when it’s not used for several hours, tenderness when kneeling, bending or climbing stairs.2
Stage 3
Classified as “moderate” degenerative arthritis. The cartilage between bones displays obvious damage, and the space between the bones is narrowing. Patients with stage 3 degenerative arthritis of the knee likely experience frequent pain when walking, running, bending or kneeling. They also may experience joint stiffness after sitting for long periods of time or when waking up in the morning. Joint swelling may be present after extended periods of motion.2
Stage 4
Considered “severe” degenerative arthritis. People in stage 4 degenerative arthritis of the knee experience great pain and discomfort when walking or moving the joint. This is because the joint space between bones is dramatically reduced — the cartilage is almost completely gone, leaving the joint stiff and possibly immobile. The synovial fluid is decreased dramatically, and no longer helps reduce friction among the moving parts of a joint.2
Altman R, Asch E, Bloch D, et al. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association. Arthritis Rheum 1986; 29:1039.
Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16(4):494-502.
50%American adults will develop
arthritis in at least one knee in
their lifetime*
Incidence and Prevalence of degenerative arthritis
In 2005 over 10% of the United States population held a clinical diagnosis degenerative arthritis, affecting 27 million Americans, and in 2009 it was the fourth most common cause of hospitalization.1 With increasing life expectancy, it is expected that the prevalence of osteoarthritis will also continue to rise.
1. Murphy, L., Helmick, CG. The impact of osteoarthritis in the United States: a population-health perspective.AM J Nurs. 2012; 112(3 Suppl 1):S13-9
MildModerateSevereMinMax
96% of total replacements
~700,000
$35 billion
Burden of degenerative arthritis
degenerative arthritis is the leading cause of disability among American adults. Because of its association with aging, prevalence of degenerative arthritis is increasing alongside the aging of the baby boomer generation. degenerative arthritis is the primary diagnosis indicated as the reason for total joint replacement surgery.
Total joint replacement is currently the definitive treatment for end-stage osteoarthritis, but it is a costly intervention and not without risk. In fact, the yearly burden of osteoarthritis has totaled $149.4 billion for insurers and $36.1 billion in out-of-pocket costs for patients.1
1. "Osteoarthritis Costs U.S. Over $185 Billion a Year." US News and World Report Health. US News and World Report LP, 2011. Web.
What is My Risk of Progression?
The most common risk factors that have been linked to osteoarthritis progression include: age, female gender, obesity, occupation, sports activities, previous injury, muscle weakness, metabolic and hormonal disorders.
Age: 4.2% of individuals from 20-39 suffer from osteoarthritis, 15.5% of adults from 40-64 suffer from osteoarthritis, and 32.5% of adults from 65 onwards suffer from osteoarthritis.1 However, studies have shown that the prevalence of degenerative arthritis is increasing in all age groups.
Gender: Females have an increased risk of the development osteoarthritis after menopause. The risk of developing degenerative arthritis for women has been estimated to be 2.6 times greater than men after adjustment for age, weight, and smoking.2,3 Women with degenerative arthritis are also more likely than men to experience rapid structural damage and to undergo total hip arthroplasty.2,3 Although advanced age and gender are not risk factors that can be prevented, awareness and management of degenerative arthritis can help reduce the severity and slow the progression of the disease.
Obesity: Excess weight adds additional pressure to the joints, leading to more bone on bone friction and cartilage loss. There is a strong association between obesity and knee osteoarthritis. Fortunately, weight loss leads to a decreased risk of the development of degenerative arthritis as well and limits its progression.4 For every pound of weight one loses, 3 to 5 pounds of force can be reduced on a joint that is standing, and 7-10 pounds of force when climbing stairs. Even a small amount of weight reduction can lead to a significantly decreased load on a diseased joint.
Occupation: Degenerative arthritis has been linked with specific occupations such as cotton workers, dock workers, shipyard workers, and carpenters.5,6 Certain occupational activities, especially those related to repetitive knee-bending and high demand activities, appear to be risk factors for the development of knee degenerative arthritis. Hip and hand degenerative arthritis have been associated with occupations that are physically intensive on the affected joint.7
Strenuous activity: Several studies have compared the prevalence of osteoarthritis (degenerative arthritis) in groups engaged in regular exercise. The following sports were associated with an increased risk of degenerative arthritis in the indicated joints.8
Wrestling (cervical spine, knees and elbows)
Boxing (carpometacarpal joints)
Pitching in baseball (shoulders and elbows)
Cycling (patellofemoral joints)
Recreational parachuting (spine, knees and ankles)
Cricket (fingers)
Gymnastics (shoulders, wrists and elbows)
Ballet dancing (talar joints)
Soccer (hips, knees, ankles, cervical spine and talar joints)
Football (knees, feet and ankles)
Previous injury: Studies have corroborated the association between existing ligamentous or meniscal injury to the knee and the subsequent risk of developing degenerative arthritis.9-12
Genetics: Unlike weight and tobacco, genetics cannot be changed by modifying one’s habits. Genes such as the VDR, AGC1, ER-alpha, TGF-beta, CRTM, and CRTL gene have all been associated with the development of osteoarthritis.13 The VDR gene is of particular interest since it codes for the vitamin D receptor in cells throughout the body. If mutated, cells may not respond properly to the presence of vitamin D, and mutations here have been shown to increase susceptibility to osteoarthritic changes.14,15 Low levels of vitamin D or improper response to vitamin D can both contribute to osteoarthritis, as there may be a reduction in mechanical compliance to physical stress, shock-absorbing capacity, and regeneration of bone. Vitamin D is crucial in calcium absorption, bone ossification, increasing bone density and bone regenerating.16 Any deficiency involving vitamin D can have dire consequences in bone formation and may exacerbate osteoarthritis risk.
Dibonaventura MD, Gupta S, Mcdonald M, Sadosky A, Pettitt D, Silverman S. Impact of self-rated osteoarthritis severity in an employed population: cross-sectional analysis of data from the national health and wellness survey. Health Qual Life Outcomes. 2012;10:30.
Davis MA, Ettinger WH, Neuhaus JM, Hauck WW. Sex differences in osteoarthritis of the knee. The role of obesity. Am J Epidemiol 1988; 127:1019.
Gelber AC, Hochberg MC, Mead LA, et al. Body mass index in young men and the risk of subsequent knee and hip osteoarthritis. Am J Med 1999; 107:542.
Maillefert JF, Gueguen A, Monreal M, et al. Sex differences in hip osteoarthritis: results of a longitudinal study in 508 patients. Ann Rheum Dis 2003; 62:931.
KELLGREN JH. Osteoarthrosis in patients and populations. Br Med J 1961; 2:1.
Cooper C, McAlindon T, Coggon D, et al. Occupational activity and osteoarthritis of the knee. Ann Rheum Dis 1994; 53:90.
Panush RS. Does exercise cause arthritis? Long-term consequences of exercise on the musculoskeletal system. Rheum Dis Clin North Am 1990; 16:827.
Mandl LA. Determining who should be referred for total hip and knee replacements. Nat Rev Rheumatol 2013; 9:351.
Boszotta H, Helperstorfer W, Kölndorfer G, et al. [Long-term results of arthroscopic meniscectomy]. Aktuelle Traumatol 1994; 24:30.
Neyret P, Donell ST, Dejour H. Osteoarthritis of the knee following meniscectomy. Br J Rheumatol 1994; 33:267.
Protect your joints Arthritis Foundation pamphlet
Phillips MJ, Krackow KA. High tibial osteotomy and distal femoral osteotomy for valgus or varus deformity around the knee. Instr Course Lect. 1998;47:429-36.Hart DJ, Spector TD. The relationship of obesity, fat distribution and osteoarthritis in women in the general population: the Chingford Study. J Rheumatol 1993; 20:331.
Spector TD, Macgregor AJ. Risk factors for osteoarthritis: genetics. Osteoarthr Cartil. 2004;12 Suppl A:S39-44.
Fernández-moreno M, Rego I, Carreira-garcia V, Blanco FJ. Genetics in osteoarthritis. Curr Genomics. 2008;9(8):542-7.
Keen RW, Hart DJ, Lanchbury JS, Spector TD. Association of early osteoarthritis of the knee with a Taq I polymorphism of the vitamin D receptor gene. Arthritis Rheum. 1997;40(8):1444-9.
Mcalindon TE, Felson DT, Zhang Y, et al. Relation of dietary intake and serum levels of vitamin D to progression of osteoarthritis of the knee among participants in the Framingham Study. Ann Intern Med. 1996;125(5):353-9.
Why Should Joint Preservation Matter to Me?
Joint preservation can prevent the progression of
osteoarthritis and involves a combination of health management, medical and surgical interventions. The goal of joint preservation is to delay or prevent the need for total joint replacement. In an ideal situation, this can be done whilst maintaining the lifestyle and activity requirements of a patient with arthritis. Although this is not always possible, the goal of MyArthritisRx is to provide the patient with the treatment and coping skills necessary to maintain activity and minimize symptoms, as well as avoid total joint replacement.
It is important to know how to correctly move your joints in order to cause the least amount of stress and cartilage damage. Simple things like changing the way you sit, stand, lie down and lift can prevent future injury and improve the overall well-being of your joints.
Nutrition and exercise play a vital role in joint preservation and should be well-managed in addition to considering medical or surgical intervention. Damage to joints can further reduce mobility, which can lead to many other problems. These problems include obesity, a sedentary lifestyle and reduced cardiovascular health, all of which can contribute to diseases like diabetes or heart attacks.
Joint preservation allows the patient to be in control of their body, gain a sense of independence and lead a healthy, active life. Too much activity, however, can lead to joint damage and it is important to take all of this into account before following a regimen.
As a member of the MyArthritisRx initiative, you can gain a better understanding of your illness, target your physical activity, plan better meal and nutritional options and perform exercises that can best improve your health. You will be given the tools to prevent or identify degenerative arthritis at its early stages, limiting the long-term severity and impact of the disease.
Treatments for Degenerative Arthritis
Self-Directed Interventions:
Over the Counter Medications
Although there is no medication that will completely cure osteoarthritis, there are therapies that alleviate pain and reduce inflammation. These medications include over-the-counter (OTC) non-steroidal anti-inflammatories (NSAIDs), nutraceuticals, glucosamine, hyaluronic acid, chondroitin, diacerein and avocado-soybean unsaponifiables.1,2
These medications have anti-inflammatory and analgesic properties to reduce pain and inflammation within the joint. Side effects of NSAID usage include the potential to develop ulcers in the stomach, leading to gastric bleeding.
Acetaminophen (Tylenol)
This is a purely pain-relieving medication with no effect on inflammation. Current guidelines recommend acetaminophen as a first-line therapy for the treatment of osteoarthritis because of the potential gastrointestinal complication that can be caused by classic NSAIDs.
Oral Glucosamine
Glucosamine is an endogenous monosaccharide working as an important precursor in the biosynthesis of glycosylated proteins, proteoglycans and lipids. In the body, it is a synthesized from glucose and used to form proteoglycans. With the progression of OA, the water content of cartilage increases as the proteoglycans within the cartilage is lost. Meta-analyses of all glucosamine studies found that when the results were pooled, glucosamine significantly reduced joint-space narrowing; however, the effect was modest.1,2
Oral Hyaluronan
Glucosamine is an endogenous monosaccharide working as an important precursor in the biosynthesis of glycosylated proteins, proteoglycans and lipids. In the body, it is a synthesized from glucose and used to form proteoglycans. With the progression of OA, the water content of cartilage increases as the proteoglycans within the cartilage is lost. Meta-analyses of all glucosamine studies found that when the results were pooled, glucosamine significantly reduced joint-space narrowing; however, the effect was modest.1,2
Oral Chondroitin Sulfate
Chondroitin sulfate comprises the majority of glycosaminoglycans in human cartilage and plays an essential role in the structural and functional integrity of the joints. Evidence from three clinical studies of patients with knee OA found that long-term treatment with chondroitin sulfate may slow joint-space narrowing.1,2
Oral Diacerein
Diacerein is believed to block the expression of cartilage-degrading enzymes.1,2
Avocado-Soybean Unsaponifiables
Avocado–soybean unsaponifiable (ASU) preparations are believed to have both antioxidant and analgesic actions.1,2
Gregory PJ, Fellner C. Dietary supplements as disease-modifying treatments in osteoarthritis: a critical appraisal. P T. 2014;39(6):436-52.
Makary MA, Segev DL, Pronovost PJ, et al. Frailty as a predictor of surgical outcomes in older patients. J Am Coll Surg. 2010;210(6):901-8.
Alternative Treatments
Mindfulness
Mindfulness is a type of meditation based on the act of living in the present moment rather than thinking about the past or the future. It has many proven benefits; patients that practice it state that it helps them understand where the pain is coming from, lowers stress levels, allows to better connect with others, improves focus on what they are doing and reduces brain clutter and internal dialogue to give relief1. In fact, patients with chronic conditions causing pain reported several benefits to their level of pain, well-being and ability to tolerate or even enjoy life again after practicing mindful meditation.1
Langer, Ellen J. Mindfulness. Da Capo Press, 2014
Yoga
Yoga has also been found to be of benefit for patients that suffer from osteoarthritis. In one study, researchers examined the effects of yoga on osteoarthritic patients receiving ultrasound and electrical stimulation treatment. Reduced pain levels, morning stiffness, state and anxiety, blood pressure and pulse were all found to be lowered in patients practicing yoga in comparison to patients that received electrical stimulation and ultrasound treatment alone17.
Ebnezar J, Nagarathna R, Yogitha B, Nagendra HR. Effect of integrated yoga therapy on pain, morning stiffness and anxiety in osteoarthritis of the knee joint: A randomized control study. Int J Yoga. 2012;5(1):28-36.
Tai Chi
Tai Chi is a traditional Chinese exercise that involves the mind and the body with the goal of improving balance, strength, flexibility and mood. It can have a variety of positive effects such as reducing pain, depression and anxiety.1 Researchers at Tufts Medical Center demonstrated that Tai Chi can benefit individuals with osteoarthritis; when asked to practice Tai Chi in bi-weekly 1-hour sessions, they found that patients had significantly reduced levels of depression, increased function and a higher sense of independence compared to individuals that were not enrolled in the sessions.2 A similar study found that Tai Chi also significantly improved balance and arthritic symptoms for women with osteoarthritis.3
Wang C, Collet JP, Lau J. The effect of Tai Chi on health outcomes in patients with chronic conditions: a systematic review. Arch Intern Med 2004; 164: 493–501.
Wang C, Schmid CH, Hibberd PL, et al. Tai Chi is effective in treating knee osteoarthritis: a randomized controlled trial. Arthritis Rheum. 2009;61(11):1545-53.
Song R, Lee EO, Lam P, Bae SC. Effects of tai chi exercise on pain, balance, muscle strength and perceived difficulties in physical functioning in older women with osteoarthritis: a randomized clinical trial. J Rheumatol. 2003;30(9):2039-44.
Acupuncture
Acupuncture is a therapy involving the insertion of fine needles at specific points in the body to facilitate stimulation and recovery. Studies have shown that it can be specifically utilized for patients with chronic pain.1,2 Several studies performed on patients with osteoarthritis demonstrated that, in addition to normal medical therapy, individuals treated with acupuncture had lower overall levels of pain and increased levels of functionality.3-5
Macpherson H, Vertosick E, Lewith G, et al. Influence of control group on effect size in trials of acupuncture for chronic pain: a secondary analysis of an individual patient data meta-analysis. PLoS ONE. 2014;9(4):e93739.
Scharf HP, Mansmann U, Streitberger K, et al. Acupuncture and knee osteoarthritis: a three-armed randomized trial. Ann Intern Med. 2006;145(1):12-20.
Plaster R, Vieira WB, Alencar FA, Nakano EY, Liebano RE. Immediate effects of electroacupuncture and manual acupuncture on pain, mobility and muscle strength in patients with knee osteoarthritis: a randomised controlled trial. Acupunct Med. 2014;32(3):236-41.
Berman BM, Lao L, Langenberg P, Lee WL, Gilpin AM, Hochberg MC. Effectiveness of acupuncture as adjunctive therapy in osteoarthritis of the knee: a randomized, controlled trial. Ann Intern Med. 2004;141(12):901-10.
Wraps, Packs, Braces and Shoe Wear
With any type of inflammation, wrapping and icing can offer considerable pain relief and inhibit further damage.
Wrapping the joint reduces swelling and prevents more fluid from concentrating within the joint space.
Icing has been shown to reduce inflammation and swelling. When inflammation and fluid collection has decreased, a heating pad is an effective means of stimulating blood flow to the affected area. With increased blood flow, the additional oxygen and healing mediators help repair the affected joint.
Bracing is also a very beneficial aspect of treatment. There are three types of knee braces commercially available for patients with degenerative joint disease: compression knee sleeves, supportive knee braces and unloading knee braces. Individuals wearing knee braces often report feeling security, support, warmth and stability.1
Compressive Supportive Unloading
Shoe wear and orthotics are also important considerations for patients with osteoarthritis. Energy-absorbing shoes with proper padding can help alleviate the impact and prevent trauma to both the knee and hip. An arch support, a calcaneal cushion and a rigid form can all help align the foot properly and improve mobility.1
Symposium I: Non-operative and Non-arthroplasty options for management of OA of the Knee. Bracing and Shoe Wear: What’s the evidence it helps? Iorio R. (Help for this citation)
Canes, Crutches, Walkers, Scooters and Wheelchairs
Mobility is one of the most important factors for individuals with osteoarthritis. As joint function decreases, normal activities such as going to the bathroom or kitchen become exceedingly difficult. With this in mind, there are a number of devices that can assist in alleviating pain, providing stability and restoring function to individuals with osteoarthritis.
The cane. Simple in construction, a cane can be made of wood, metal or plastic. Canes offer balance and redistribute weight to better suit a person’s needs and have been shown to significantly reduce pain levels, increase mobility and raise quality of life in patients.1
Crutches are other useful assistance devices that can help people get around. There are four basic types: the forearm crutch, underarm crutch, platform crutch and leg support crutch.
The forearm crutch allows individuals to insert their arms in a sleeve and then grip onto a handle.
The underarm crutch, or axillary crutch, is usually propped under the arm in the armpit.2
The platform crutch utilizes a surface on which the forearm can rest.
The leg support crutch supports the lower leg and these can come equipped with wheels to allow patients to slide their affected leg forward rather than lift it.
Forearm Crutch Underarm CrutchPlatform Crutch Leg Support Crutch
Walkers can offer support to both sides of the body. They allow patients to lean forward and move at their own pace. Scooters and wheelchairs can also provide mobility for patients with minimal exertion. Scooters tend to be battery powered and individuals simply sit on them and drive around, similar to a car.
Wheelchairs can be electric, similar to scooters, or manual. While electric scooters and wheelchairs can significantly ease the burden of motility for individuals, the downside of these devices is their reliance on electric power. Manual wheelchairs can be operated by either the person sitting on the chair or through assistance from a caregiver.
Walker Scooter Manual Wheelchair Electric Wheelchair
Jones A, Silva PG, Silva AC, et al. Impact of cane use on pain, function, general health and energy expenditure during gait in patients with knee osteoarthritis: a randomised controlled trial. Ann Rheum Dis. 2012;71(2):172-9.
Mcfall B, Arya N, Soong C, Lee B, Hannon R. Crutch induced axillary artery injury. Ulster Med J. 2004;73(1):50-2.
Ergonomics
It’s possible to manage and minimize the effects of your OA by listening to what your body needs. The Arthritis Foundation promotes a system of self-reflection and correction that minimizes the effects of OA and the first step here is to check your posture.
Your posture changes depending on whether you are standing, sitting or lying down and you may find that any one of these aggravates your pain. Use these guidelines to adjust your posture, putting your body under as little stress as possible.1
Position
Posture
Additional support
Standing
Stand upright, with feet a shoulder width apart.
Shoulders back and abdominal muscles tightened.
Knees should be straight, but not locked.
Try leaning against a wall, or putting your foot on a lower stool to relieve pressure on joints.
Sitting
Sit tall, with feet planted on the floor or footrest.
Hips, knees and ankles should be at a 90 degree angle.
Relax shoulders and bend arms at the elbow.
A computer or book should be at eye level.
Place a pillow or rolled up towel between your lower back and the chair behind you.
Lying Down
Lie on your back, with a pillow or rolled up towel underneath your neck.
If lying on your side, hold a pillow between your knees.
Avoid pillows underneath your knees – this can cause tightening of muscles.
Pressure from everyday activities can be unavoidable, but there are ways that you can relieve this. Think of your joints like any other part of your body: you need to warm them up to loosen them. Getting up and moving around every 15 minutes can help prevent discomfort.
It is also important to complete a movement check of your jaw, neck, shoulders, arms, wrists, fingers, hips, legs, ankles and toes. These joints are prone to stiffness and you may not notice the pain until it becomes severe. Stretch and relax areas of your body that feel stress.1
If you’re handling heavy loads, distribute the weight of the load over the larger, stronger joints to reduce stress on the smaller joints. Use the palms of your hands, rather than gripping with your fingers and hold the item close to your body. Wherever possible, have another person help you or slide the load instead of lifting it.1
“Ergonomics.” Safety Office. University of Waterloo, 14 May 2015. Web. 16 Dec. 2015.
Physical Therapy
Physical therapy is a unique part of your treatment. Your therapist can guide you through specific exercises that can alleviate symptoms and strengthen surrounding muscles and there are many studies that show the benefits:
The Evidence | Physical Therapy Trial
Outline
A group of patients with knee osteoarthritis were asked to do an exercise on their own, while another group did this under the guidance of a physical therapist.
Findings
Both groups reported lower levels of pain. However, a comparison of pain scores showed that the supervised patients had twice the level of improvement.23.
Takeaway
Patients treated with manual physical therapy reported both significant improvements in self-perception of pain, stiffness and functional ability. They could also walk further in a given amount of time. 24.
Deyle GD, Henderson NE, Matekel RL, Ryder MG, Garber MB, Allison SC. Effectiveness of manual physical therapy and exercise in osteoarthritis of the knee. A randomized, controlled trial. Ann Intern Med. 2000;132(3):173-81.
Physician-Prescribed Medications/Therapies
If it hasn’t been possible to relieve your symptoms through self-management, you may want to explore prescribed medications and therapies. Here’s a guide to some of the options available to you.
Cox-2 inhibitor (Celecoxib)
A nonsteroidal anti-inflammatory medication (NSAID) used to reduce inflammation and relieve pain
Targets the inflammatory pathway specifically so that you can avoid gastrointestinal complications.
Potential complications include blood clots, heart attacks and stroke
Hyaluronic Acid (HA) Injection
A fluid injected directly into the joint, that promotes functional improvement and reduces pain
This is a naturally occurring substance found in synovial fluid that helps lubricate joints
Platelet-rich Plasma
A platelet injection directly into the joint
Platelets assist with clotting when injury occurs and encourage growth and healing
Stem-cells
Stem-cells from a living adult donor are injected directly into the joint.
Studies show that the stem-cells may grow into cells that become part of the musculoskeletal system, replacing what the body has lost.2
Corticosteroid Injections (Cortisone Shot)
Anti-inflammatory injections are used widely for rapid pain relief and increasing functionality.
Injections are limited to a maximum of once every 3 months. This prevents tendon weakening, thinning of nearby bone and skin and crystallization.
Narcotics (Norco, Vicodin, Demerol, Oxycodone)
Narcotics are used for uncontrollable pain.
Associated risks are respiratory depression, decreased heart rate, addiction, withdrawal and tolerance necessitating higher doses to adequately control pain.
Orthoinfo.aaos.org. Stem Cells and Orthopaedics-OrthoInfo - AAOS. 2007. Available at: http://orthoinfo.aaos.org/topic.cfm?topic=A00501. Accessed December 9, 2015.
Treatments can help you manage your symptoms effectively. In some cases, surgery may be the only way to control your pain, help with functionality and improve your quality of life. Surgical intervention has been proven to be very effective. As with all invasive procedures, there are risks involved. The LIMA program can help you to:
delay surgery for as long as possible
prevent revision surgery
optimize your health prior to surgery
Joint Preservation Surgeries
Osteotomy:
A surgery involving redirection of the misaligned part of the joint that can help by “unloading” the affected area and adjusting the lines of force. This is generally recommended to younger, active patients who are affected by arthritis in only one part of their knee. It’s also a resolution for “bowleg” or “knock knee”. Osteotomy has been shown to benefit the patient by relieving pain and improving and preserving functionality.1
Joint Resurfacing:
A surgical treatment involving the resurfacing of the joint. In the hip, the ball and socket are resurfaced, creating a smooth metal surface.2 This is an alternative to total hip replacement, which preserves more of the bone. In the knee, the patella and trochlea can be resurfaced to treat patellofemoral osteoarthritis.
Joint Replacement Surgeries
Partial Joint Arthroplasty:
For patients affected by OA in only one area of the knee, a uni-compartmental arthroplasty (UKA) can be an effective alternative to a total knee arthroplasty. The comparative benefits typically include a quicker recovery time and improved range of motion. It may also feel more like your original knee.3 The procedure is generally recommended over joint realignment for younger patients or for older patients.4, 5
For those affected by arthritis in the hip, a “hemiarthroplasty” replaces the ball and stem of the femur without replacing the socket on the pelvis. This is usually suitable for older people with a femoral neck fracture, rather than osteoarthritis.6
Total Joint Arthroplasty:
This is generally the final intervention for severe, end stage arthritis and involves removing and replacing the joint with a prosthetic. It’s proven to be an effective surgery, reducing pain and improving function and improving your quality of life for years to come. 7
Revision Arthroplasty:
A revision surgery may be required as a fix if there are complications associated with the prosthetic implant, or if the prosthetic is worn passed its average lifespan of around 15-30 years.
Corten K, MacDonald SJ. Hip resurfacing data from national joint registries: what do they tell us? What do they not tell us? Clin Orthop Relat Res 2010; 468:351.
Bert JM. Unicompartmental knee replacement. Orthop Clin North Am. 2005;36(4):513-22.
Brown NM, Sheth NP, Davis K, Berend ME, Lombardi AV, Berend KR, Della Valle CJ. Total knee arthroplasty has higher postoperative morbidity than unicompartmental knee arthroplasty: a multicenter analysis. J Arthroplasty. 2012 Sep;27(8)(Suppl):86-90
Ghomrawi HM, Eggman AA, Pearle AD. Effect of age on cost-effectiveness of unicompartmental knee arthroplasty compared with total knee arthroplasty in the U.S. J Bone Joint Surg Am. 2015;97(5):396-402.
Parker MJ. Hemiarthroplasty versus internal fixation for displaced intracapsular fractures of the hip in elderly men: a pilot randomised trial. Bone Joint J. 2015;97-B(7):992-6.
Mandl LA. Determining who should be referred for total hip and knee replacements. Nat Rev Rheumatol 2013; 9:351.
Panush RS. Does exercise cause arthritis? Long-term consequences of exercise on the musculoskeletal system. Rheum Dis Clin North Am 1990; 16:827.
Perioperative Orthopedic Surgical Home (POSH)
As a candidate for joint replacement, POSH is a diagnostic tool used to assess your risk. The goal is to prepare you for surgery and the program offers clinical treatments and interventions designed to mitigate risk factors. Here’s an outline of the risk factors, how these may affect you and the interventions that can benefit you ahead of surgery:
Morbid obesity
Poorly controlled diabetes
Malnutrition and hyperglycemia
Smoking
S Aureus colonization
Cardiovascular disease
Venous thromboembolic disease
Neurocognitive, psychological and behavioral problems (including drug and alcohol dependency)
Physical deconditioning of comorbidities affecting mobility and fall risk
POSH Interventions to Minimize Modifiable Risk Factors:
MRSA Screening and Decolonization, weight based antibiotic dosing and use of Vancomycin and Gentamycin in high risk patients
Hepatitis C screening and treatment
Smoking cessation
Cardiovascular Optimization and Stroke Prevention (using PT, High dose Statins and ACE inhibitors perioperatively)
Diabetes control and nutritional interventions (Hard Stop with glucose > 180)
Frailty assessment
Smoking Cessation
Tobacco dependence is a leading cause of death in the US. 21-24% of patients undergoing THA or TKA are current users1,2 and (both current and former users) have a 56% higher risk of post-operative complications. Pre-operative tobacco cessation programs begin 6-8 weeks prior to surgery and reduce risk, particularly of wound-related complications. This kind of intervention can lead to a better outcome from the surgery as well as improving your overall health.1
Singh J, Houston T, Ponce B, Maddox G, Bishop M, Richman J, Campagna E, Henderson W, Hawn M. Smoking as a risk factor for short-term outcomes following primary total hip and total knee replacement in veterans. Arthritis Care Res (Hoboken). 2011; 63(10):1365-74.
Kapadia B, Johnson A, Naziri Q, Mont M, Delanois R, Bonutti P. Increased revision rates after total knee arthroplasty in patients who smoke. The Journal of Arthroplasty. 2012; 27(9):1690-96.
Sadr azodi O, Bellocco R, Eriksson K, Adami J. The impact of tobacco use and body mass index on the length of stay in hospital and the risk of post-operative complications among patients undergoing total hip replacement. J Bone Joint Surg Br. 2006;88(10):1316-20.
Cardiovascular Optimization and Stroke Prevention
A significant proportion of patients who undergo total joint replacement are older, so the risk of cardiovascular complication (including myocardial infarction-MI) is relatively high (0.8% within 90 days). Managing cardiovascular risks preoperatively may lead to fewer complications1.
Katz JN, Barrett J, Mahomed NN, Baron JA, Wright RJ, Losina E. Association between hospital and surgeon procedure volume and the outcomes of total knee replacement. J Bone Joint Surg Am. 2004;86-A(9):1909-16.
Obesity
Obese patients undergoing total joint replacements experience improvements in mobility, pain and lower limb function. However, they’re also at risk of immediate and long-term post-operative complications including infection (superficial and deep). Longer operating time, difficult surgical exposure, decreased vascularization of fatty tissue and weakened immune response may contribute to increased infection rates. Obese patients also experience less significant improvements when compared to their non-obese counterparts.
Recovery may also be slower and more difficult for obese patients, who tend to have higher pain scores ahead of undergoing total joint replacement. Increased nutritional deficiencies and risk of postoperative infection have been observed. Weight loss can delay surgical intervention and can promote joint and overall health in an arthritic patient.1-3
Vasarhelyi EM, MacDonald SJ. The influence of obesity on total joint arthroplasty. J Bone Joint Surg Br. 2012; 94-B(A):100-2.
Kerkhoffs GMMJ, Servien E, Dunn W, Dahm D, Bramer JAM, Haverkamp D. The influence of obesity on the complication rate and outcome of total knee arthroplasty: a meta-analysis and systematic literature review. J Bone Joint Surg Am. 2012; 94(20):1839-44.
Gillespie GN, Porteous AJ. Obesity and knee arthroplasty. Knee. 2007; 14(2):81-6.
Psychological, Neurocognitive, Pain Management and Substance Problems
Emotional responses to pain are also related to the outcome of a surgery. It is important that these are included in a pre-surgical risk modification program. Pain, especially when catastrophically expressed, is an important psychological issue associated with osteoarthritis. Depression and catastrophizing can also mean a longer hospital stay.1
Management includes: educating patients about arthritis and hip function; cognitive behavioral methods; and relaxation techniques. All of these can result in reducing the patient’s experience of pain.2 Cognitive-behavioral techniques (derived from psychotherapy) have been developed specifically to address psychological risk factors in patients with musculoskeletal injuries. This approach increases the patient’s sense of self-efficacy and control over pain, reduces pain-related distress and replaces focus on pain with meaningful activities. 3 Improved pain management may also be a way for you to delay the need for invasive intervention.
Post-operative cognitive decline (POCD) is also associated with increased mortality, as well as prolonged time spent in hospital. 4-6 An example is delirium (characterized by fluctuating consciousness and inattention), which has been reported in elderly patients undergoing elective orthopaedic surgery at a rate of between 9-28%. Risks associated with POCD include age, gender, pre-operative cognitive impairment (i.e. dementia) as well as a history of alcohol abuse and narcotic use.6,8,9 It may be possible to reduce the risk of POCD through treatment of alcohol abuse and managing pre-operative narcotic use.
Alcohol abuse is an independent risk factor. Patients with a history of alcohol and drug abuse are likely to have trouble with pain control. They may also develop complications (pneumonia, sepsis, PE and infection) that mean a longer hospital stay and can limit rehabilitation.10,11 Treating alcohol and drug abuse ahead of surgery can mean a better outcome for the patient.
Witvrouw E, Pattyn E, Almqvist KF, Crumbez G, Accoe D, Cambier D, Verdonk R. Catastrophic thinking about pain as a predictor of length of hospital stay after total knee arthroplasty: a prospective study. Knee Surg Sports Traumatol Arthrosc. 2009; 17:1189-94.
Berge DJ, Dolin SJ, Williams AC, Harman R. Pre-operative and post-operative effect of a pain management programme prior to total hip replacement: A randomized controlled trial. Pain. 2004; 110:33-39.
Hofmann SG. An introduction to modern CBT : psychological solutions to mental health problems Chichester, West Sussex, U.K. ; Malden, MA: Wiley-Blackwell; 2012.
Jankowski CJ, Trenerry MR, Cook DJ, Buenvenida SL, Stevens SR, Schroeder DR and Warner DO. Cognitive and Functional Predictors and Sequelae of Postoperative Delirium in Elderly Patients Undergoing Elective Joint Arthroplasty. Analgesia & Anaesthesia. 2011; 112(5):1186-1193.
Terrando N, Brzezinski M, Degos V, Eriksson LI, Kramer JH, Leung JM, Miller BL, Seeley WW, Vacas S, Weiner MW, Yaffe K, Young WL, Xie Z, Maze M. Perioperative cognitive decline in the aging population. Mayo Clin Proc. 2011; 86(9):885-93.
Marcantonio ER, Goldman L, Mangione CM, et al. A Clinical Prediction Rule for Delirium After Elective Noncardiac Surgery. JAMA. 1994; 271(2):134-139.
Bruce AJ, Ritchie CW, Blizard R, Lai R, Raven P. The incidence of delirium associated with orthopedic surgery: a meta-analytic review. Int Psychogeriatr. 2007; 19(2):197-214.
Litaker D, Locala J, Franco K, Bronson DL, Tannous Z. Preoperative risk factors for postoperative delirium. Gen Hosp Psychiatry. 2001; 23(2):84-9.
Williams-Russo P, Urquhart BL, Sharrock NE, Charlson ME. Post-operative delirium: predictors and prognosis in elderly orthopedic patients. J Am Geriatr Soc. 1992; 40(8):759-67.
Rubinsky AD, Sun H, Blough DK, Maynard C, Bryson CL, Harris AH, Hawkins EJ, Beste LA, Henderson WG, Hawn MT, Hughes G, Bishop MJ, Etzioni R, Tønnesen H, Kivlahan DR, Bradley KA. AUDIT-C alcohol screening results and postoperative inpatient health care use. J Am Coll Surg.2012; 214(3):296-305.
Harris AH, Reeder R, Ellerbe L, Bradley KA, Rubinsky AD, Giori NJ. Preoperative alcohol screening scores: association with complications in men undergoing total joint arthroplasty. J Bone Joint Surg Am. 2011; 93(4):321-7.
Physical Deconditioning and Comorbidities Affecting Ambulation
Patients with ambulatory mobility problems are also at risk for longer rehabilitation and stay in hospital. Pre-operative conditioning training, or “prehabilitation”, can help with function and independence following surgery. It’s been shown to reduce length of stay and hospital readmission for patients with pre-existing issues. Balance disorders and neuromuscular conditions that affect ambulation can also improved with “prehab programs”.1
Rooks DS, Huang J, Bierbaum BE, Bolus SA and Rubano J. Effect of preoperative exercise on measures of functional status in men and women undergoing total hip and knee arthroplasty. Arthritis & Rheumatism. 2006; 55(5):700-708.
Fall Prevention
Evaluating risks within the home and putting fall risk prevention strategies in place ahead of surgery can also help prevent readmissions. Physiotherapy programs for patients with hip or knee osteoarthritis can relieve pain and increase functionality. This may include some form of physical therapy and education and can reduce a patient’s hospital stay as well as the risk of complications and readmissions.
Johnson RL, Duncan CM, Ahn KS, Schroeder DR, Horlocker TT, Kopp SL. Fall-Prevention Strategies and Patient Characteristics That Impact Fall Rates After Total Knee Arthroplasty. Anesthesia and Analgesia 2014 Sep 10. Epub.
Ackerman DB, Trousdale RT, Bieber P, Henely J, Pagnano MW, Berry DJ. Postoperative Patient Falls on an Orthopedic Inpatient Unit. Journal of Arthroplasty 2010. 25(1):10-14
Diabetes Complications and Nutritional Deficiencies
8% of patients undergoing total joint replacement in the US have a diagnosis of Diabetes mellitus (DM) Types I and II and those with uncontrolled DM are more likely to experience complications. Total joint replacement patients are at a greater risk of cerebrovascular accident (CVA), urinary tract infection (UTI), paralytic ileus, infection, post-operative hemorrhage, transfusion and death.1-4
Marchant Jr MH, Viens NA, Cook C, Vail TP, Bolognesi MP. The impact of glycemic control and diabetes mellitus on perioperative outcomes after total joint arthroplasty. J Bone Joint Surg Am. 2009;91(7):1621-9.
Iorio R, Williams KM, Marcantonio AJ, Specht LM, Tilzey JF, Healy WL. Diabetes mellitus, hemoglobin A1C and the incidence of total joint arthroplasty infection. J Arthroplasty. 2012;27(5):726-9.e1.
Adams AL, Paxton EW, Wang JQ, Johnson ES, Bayliss EA, Ferrara A, Nakasato C, Bini SA, Namba RS. Surgical outcomes of total knee replacement according to diabetes status and glycemic control, 2001 to 2009. J Bone Joint Surg Am. 2013; 95(6):481-7.
Bolognesi MP, Marchant MH, Viens NA, Cook C, Pietrobon R, Vail TP. The impact of diabetes on perioperative patient outcomes after total hip and total knee arthroplasty in the United States. J Arthroplasty. 2008; 23(6 Suppl 1):92-8.
Frailty
Frailty is a measure of your physiologic reserves and is experienced by many elderly patients. Reserves can be used up during periods of stress like undergoing surgery and may affect how a patient responds to a procedure. A study by Makary et al. defines frailty as weakness, weight loss, exhaustion, low physical activity and slow walking speed. They found that preoperative frailty was associated with an increased risk for postoperative complications and length of hospital stay.1
Tevis SE, Kennedy GD. Postoperative complications and implications on patient-centered outcomes. J Surg Res. 2013;181(1):106-13.
Glossary
All-natural: Does not contain synthetic or artificial ingredients.
Antibody: A molecule made by the body that works as a “tag” on other molecules and marks them for destruction by the immune system.
Biomarkers: Molecules found in tissue that can provide information about the tissue or the person. For example, cholesterol is used to determine whether a patient needs cholesterol-lowering medication.
Cartilage: A type of tissue that provides a viscoelastic, shock-absorbing matrix at the ends of bones. Cartilage allows bones to rub against each other in a non-damaging way.
Cholesterol-free: Containing less than 2mg cholesterol per serving and 2 grams or less of saturated fat per serving.
Chondroitin sulfate: A molecule naturally found in cartilage. This a mixture of protein and carbohydrate and is disputed as either beneficial or unbeneficial when taken over the counter as a supplement.
Collagen: One of the most abundant proteins in the human body and a key property of cartilage. It is capable of stretching and absorbing shock.
Corticosteroid: A molecule that the body can produce, which can also be injected into tissues to prevent inflammation. Can provide instant relief to patients that have symptoms of pain and swelling.
Fat-free: Less than 0.5 grams of fat per serving, with no added fat or oil.
Gluten-free: Less than 20 parts per million of gluten.
High Potency: Individual vitamins or minerals that are present at 100% RDI.
High-fiber: 5 grams or more of fiber per serving.
High/Rich in/Excellent: Contains 20% or more of the recommended daily intake (RDI).
Hyaluronic Acid: A molecule found in high quantities in synovial fluid. This molecule helps the synovial fluid provide lubrication for joints and allows bone surfaces and cartilage to glide on each other.
Joint: This is the union of two bones. There are several types of joints; some such as the knee joint and the hip joint allow for a lot of movement, while others such as the joints between the bones in the skull don’t allow for much movement at all.
Less fat: 25% or less fat than the comparison food.
Low cholesterol: 20 mg or less cholesterol per serving and 2 grams or less saturated fat per serving.
Low fat: 2 grams of fat or less per serving.
Low sodium: 140mg or less per serving.
Non-steroidal Anti-inflammatory Drug: A type of drug that prevents inflammation. Common examples include aspirin and ibuprofen. These drugs work by stopping certain processes in the body that lead to inflammation. NSAIDs can relieve pain, swelling, redness and heat production in areas of inflammation.
Organic: Food meets standards set by the U.S Department of Agriculture.
Viscoelastic: A property of materials that exhibit both viscous and elastic characteristics when undergoing deformation.
Ready For Change?
Sign up today to join the many individuals who will defeat the symptoms of arthritis through our step-by-step program. With the applied sciences of innovative technologists and medical industry professionals, you can once again experience life free of the overwhelming burden of chronic joint pain.
Register
Stay Active
Enjoy your daily activities knowing you are in control of your arthritis
Sign In
Register
If you are not a member, please Click
Here to enroll